



Supporting disabled war refugees from Ukraine in the UK
Our work involves in-depth interviews and surveys in both the UK and Ukraine with Ukrainians with disabilities.
In the UK we aim to improve the lives of Ukrainian war refugees with disabilities and promote pathways for longer-term settlement for this group.
In Ukraine we aim to help those with disabilities by supporting emergency protection during the war and identify ways to support longer-term reconstruction.
Background
- Large-scale survey data collected in Ukraine during the initial weeks of the conflict showed a significant association between having a disability and post-traumatic distress.
- Later work with nearly 10000 displaced Ukrainians across Europe found those with visual or mobility difficulties reported greater anxiety and poor sleep.
- In the UK more than 250,000 visas have been issued by the Home Office under the Ukraine schemes. Approximately 15% of new arrivals reported significant physical or mental health conditions, with 32% receiving healthcare treatment before leaving Ukraine. However, we know little about the particular challenges faced by Ukrainian war refugees with disabilities in the UK.
- The number of persons with disabilities in Ukraine has risen significantly since 2022. Many face deepening poverty, low levels of employment (only 17% are formally employed), poor housing, and severe disruptions to social care and rehabilitation.
Our work
- We conducted the first UK research focused specifically on physically disabled Ukrainian war refugees.
- During in-depth interviews in the UK we questioned 45 Ukrainian war refugees with physical and sensory disabilities. Research questions included the journey to the UK, subsequent housing, work, education, welfare, healthcare, social relations, and mental health. Results are reported below.
- In a companion survey in the UK (ongoing) we are using a structured questionnaire to explore these issues, employing a further sample of refugees with physical and sensory disabilities. So far, we have 200 completed surveys but are still collecting data. You can participate here. (Analysis is currently ongoing and will be reported below).
- In Ukraine, we are also working with adults with physical disabilities and caregivers, including war veterans. In online interviews and focus groups we questioned 51 disabled respondents in this country on how the war has affected access to rehabilitation, healthcare, housing, employment, and independent living. (Analysis is currently ongoing and will be reported below).
Figure 1: Origin of disabled Ukrainian war refugees in our UK interview sample

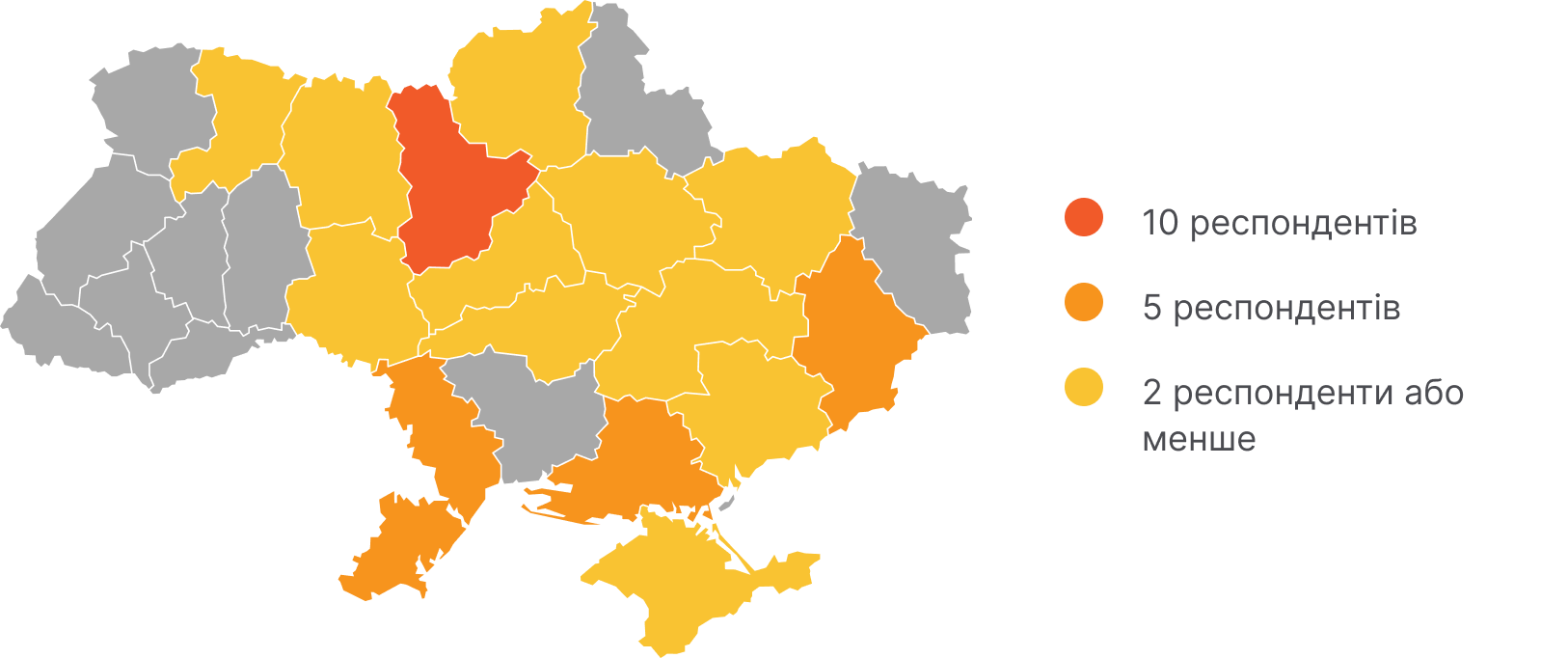

10 respondents
5 respondents
2 respondents or less
Scroll

Impact of the war on cities
City / oblast
Total
Active hostilities / destroyed / occupied cities
Donetsk (city & oblast) (5), Zaporizhzhia (city & oblast) (2), Kherson (city & oblast) (5), Crimea (1)
13
Cities subject to regular air strikes
Kyiv (city & oblast) (10), Kharkiv (city & oblast) (2), Chernihiv (2), Dnipro (2), Odesa (5)
21
Peripheral areas affected by indirect hostilities (occasional air strikes)
Vinnytsia (1), Zhytomyr (1), Cherkasy (1), Poltava (1), Rivne (1), Kropyvnytskyi (1)
6
Not specified
(5)
5
City / oblast
Impact of the war on cities
Total respondents
Donetsk (city & oblast), Zaporizhzhia (city & oblast), Kherson (city & oblast), Crimea
Active hostilities / destroyed / occupied cities
13
Kyiv (city & oblast), Kharkiv (city & oblast), Chernihiv, Dnipro, Odesa
Cities subject to regular air strikes
21
Vinnytsia, Zhytomyr, Cherkasy, Poltava, Rivne, Kropyvnytskyi
Peripheral areas affected by indirect hostilities (occasional air strikes)
6
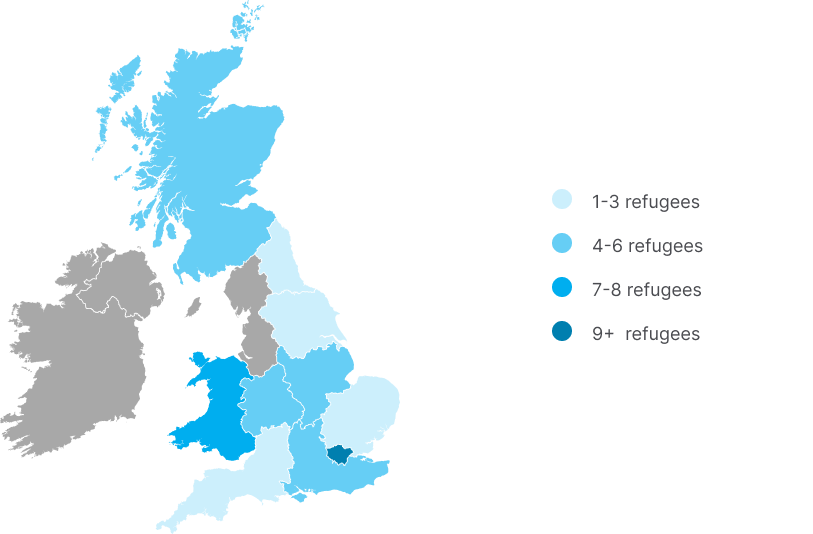
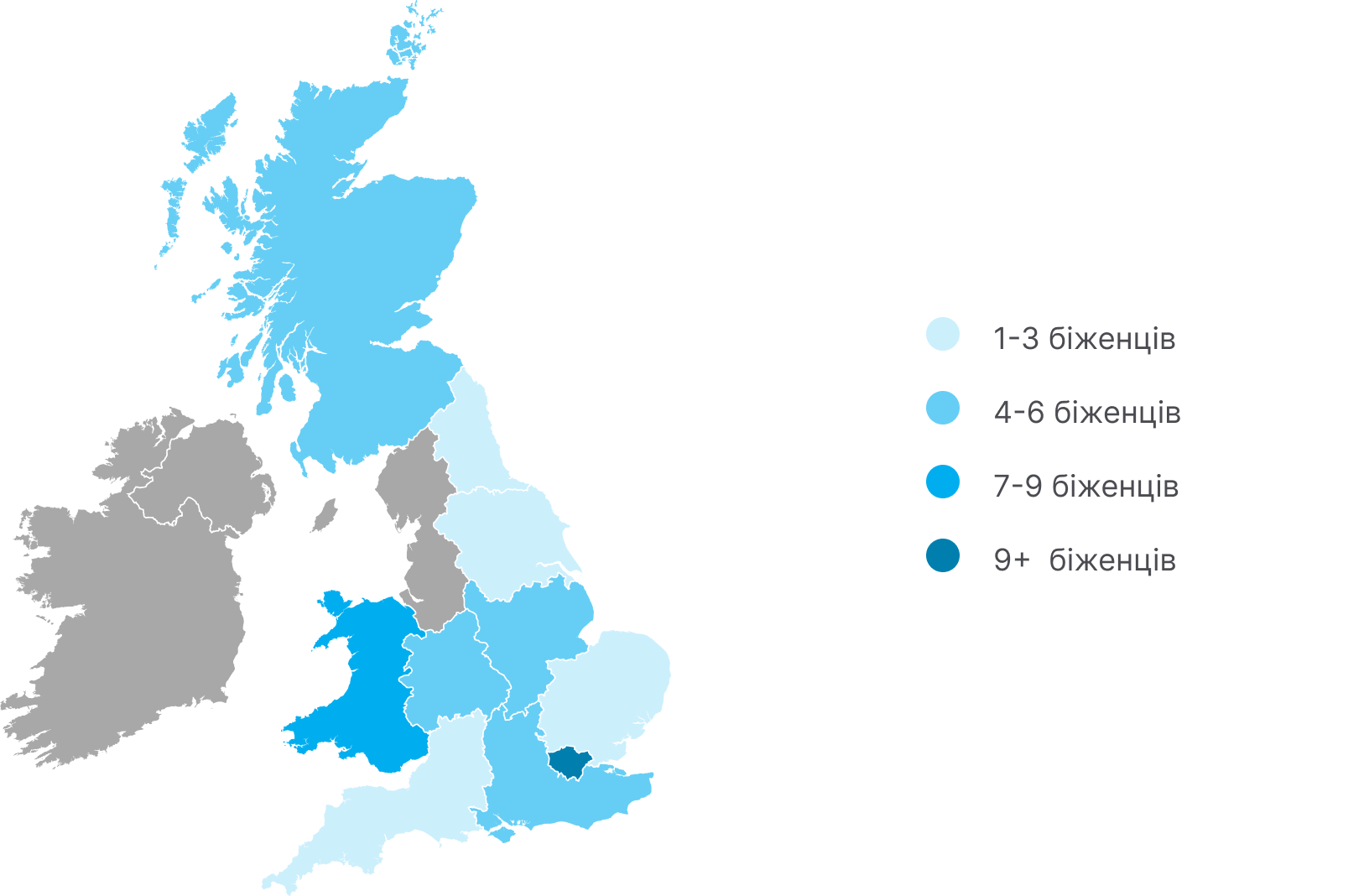
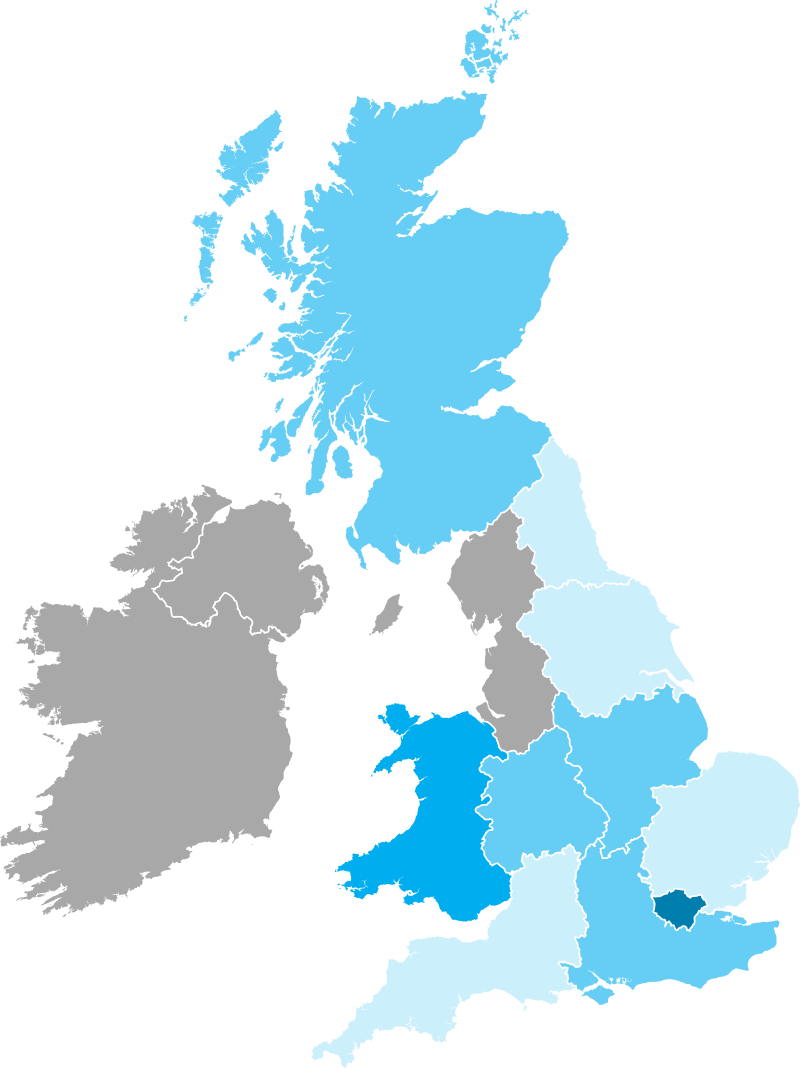
Figure 2: Current UK residence of our interview sample
UK region
Places included
Total
London
London, Croydon
9
Wales
Cardiff, Carmarthen
7
West Midlands
Birmingham, Solihull, Coventry, Warwick
6
Scotland
Glasgow, Edinburgh
5
South East England
Oxfordshire, Reading, Brighton, Eastbourne
5
East Midlands
Nottingham, Sheffield
4
Yorkshire & the Humber
Leeds, North Yorkshire
2
South West England
Bristol, Truro
2
North East England
Newcastle
1
East of England
Fakenham
1
Not specified
-
3
Total
45
1-3 refugees
4-6 refugees
7-8 refugees
9+ refugees
Stability and Settlement for Disabled Ukrainian Refugees
Robin Goodwin, Tarandeep Kang, Olena Orlova, University of Warwick
Key findings in the UK
- Uncertainty about the opportunity to remain long-term in the UK is an important impediment to the employment, housing, and well-being of all Ukrainian refugees in the UK, but these challenges are particularly severe for those with disabilities.
- UK rehabilitation, specialist care, mobility aids and disability-inclusive services are unavailable or unsafe in Ukraine: “ … when Russia came, we did not use state services at all… ” (Antonina, on behalf of a disabled child with cerebral palsy, wheelchair user)
- Despite a strong motivation to work, inappropriate JobCentre referrals and delays in receiving clinical assessments and rehabilitation led many unable to engage in employment: “I’m visually impaired... the job centre... sent me to be a bus driver. ” (Victoria)
- Depression, anxiety and social isolation were common in this group. This reduced work-readiness, especially for those in rural areas or without peer/community networks: “I still have depression... this is one of the reasons why I can't find a job now. I just pass out for a few days... ” (Mykola, connective tissue dysplasia)
- Some with disabilities require financial support. However complex English-only forms and inconsistent professional advice led many eligible participants to abandon applications: “ …it was difficult for me here to organise it at first with the language barrier... with the lack of support for special children with disabilities. ” (Valeriia, parent of a child with vision impairment)
- Moves between temporary accommodations and a lack of accessible housing reduced stability and interrupted care: “nothing even goes here except taxis... it’s a lot of money... if I need to go to the neurologist I need the bus... a healthy person can get there in 5-6 minutes, it takes me half an hour. ” (Olga, MS)
Recommendations in the UK

Participants consistently described an “information vacuum” during their first months / year in the UK. Many struggled to understand how to access disability-related benefits, NHS entitlements (including rehabilitation and medication), GP services, and available mobility schemes. Language barriers and unfamiliarity with the British welfare and healthcare systems, which differ significantly from the Ukrainian system, led to uncompleted benefit applications, delays in accessing healthcare, poor advice from professionals, and in some cases incorrect benefit decisions due to staff assessment errors, resulting in refusals and delays of up to a year before being corrected.
We recommend providing every Ukrainian refugee with physical disabilities with a short, translated guide explaining disability benefits, GP and NHS access, rehabilitation, medication, and mobility support. This should be given through local councils, Job Centres, GP practices, NHS services, and the Department for Work and Pensions teams. They should also be referred straight away to a Ukrainian-speaking support organisation, with access to interpreters and, where needed, specialist legal advice for difficult immigration or benefits cases. Funding should be increased for organisations such as Settled and OPORA so they can provide this support consistently.
In our research with disabled Ukrainian refugees respondents identified particular challenges with PIP assessments. These assessments require detailed medical evidence (e.g. specialist reports, formal diagnoses, supporting letters from healthcare professionals). Many Ukrainian refugees with physical disabilities fled without complete medical records or hold documentation that is not translated into English. As a result, they are often unable to provide the level of evidence typically expected in UK assessments. While a UK-born applicant may submit comprehensive specialist reports, a refugee may only have a brief GP note or supporting letter from a voluntary organisation, which may be viewed as insufficient. This creates a significant barrier to accessing disability-related benefits, even where eligibility criteria are met.
Language barriers further complicate the process. PIP forms and official communications use complex administrative and medical terminology, which can be difficult to understand even for fluent English speakers. When claims are delayed or refused, applicants are often required to make follow-up phone calls, request mandatory reconsiderations, or respond to further queries. For individuals with limited English, hearing impairments, or communication difficulties, managing these phone-based interactions can be particularly challenging. This increases the risk of incomplete applications, unchallenged refusals, or incomplete claims.
We recommend funding translation of medical documents and key benefit paperwork, and funding voluntary sector organisations to help Ukrainian refugees with physical disabilities complete claims, respond to refusals, and request reconsideration where needed. The Department for Work and Pensions staff should also be allowed to accept Ukrainian medical evidence, translated summaries, and supporting letters where full records are missing because of war and displacement.
Housing was one of the most significant structural barriers identified in our research. Participants were placed in accommodation that did not meet their physical needs, including multi-storybuildings without lifts, upper-floor flats unsuitable for people with mobility impairments, elderly individuals in inaccessible housing, and a family with a wheelchair-using child placed on a ship.
These placements directly restricted access to rehabilitation, medical appointments, Job Centre training, interviews, and community support. Many participants were placed in rural or poorly connected areas, limiting their ability to access healthcare, employment, and social networks.
Transport barriers further increased isolation. Participants reported long distances to bus stops, unreliable services, taxi costs of £25-30 per trip, and limited awareness or access to mobility schemes. For some, reaching public transport took significantly longer due to mobility impairments. These barriers reduced work-readiness, affected mental health, and disrupted healthcare continuity.
We recommend that when a Ukrainian refugee declares a physical, visual, hearing, or long-term health condition, a disability housing assessment is carried out before placement. Housing should be checked for lift access, proximity to healthcare, transport links, and access to rehabilitation or employment services. Ukrainian refugees with physical disabilities should not be placed in remote or poorly connected areas unless reliable transport support is in place. Where housing cannot be changed, local councils should provide transport support for medical appointments, work, and essential services.
Participants consistently expressed strong motivation to work. However, many encountered inappropriate job referrals that did not reflect their functional limitations. For example, a visually impaired participant was advised to apply for a bus driver role, and a person with hearing loss was scheduled for a phone-based appointment despite stating this was not manageable.
These examples indicate a lack of individualised assessment and insufficient understanding of disability-related needs within employment services.
We recommend that Ukrainian refugees with physical disabilities are referred directly to Disability Employment Advisers rather than standard pathways. Job Centre staff should check communication needs, functional limitations, and medical restrictions before assigning appointments or suggesting jobs. Interpreters should be available where needed, and appointment formats should be adjusted for hearing, visual, or mobility impairments.
Many participants described depression, anxiety, trauma, and social isolation that directly affected their ability to work and integrate. NHS / GP mental health services were often experienced as difficult to access due to language barriers and limited availability of culturally appropriate support. Services were frequently perceived as focused on short-term or low-intensity interventions, which were not sufficient for individuals experiencing persisting war-related traumas or complex health needs.
Our participants reported that when GP referrals did not result in appropriate psychological support, they sought help informally from Ukrainian psychiatrists. Participants consistently emphasised the importance of speaking to psychologists who speak Ukrainian and understand their cultural and war-related experiences.
Despite this need, Ukrainian psychologists in the UK often do not pursue full UK qualification because the process takes 3-4 years while visa status remains uncertain. As a result, there is a significant unused professional capacity within the Ukrainian community. Those Ukrainian psychologists who have already obtained UK recognition report limited funding and are unable to meet demand.
At present, support is partly provided by Ukrainian-led organisations. For example, the UK-registered charity OPORA delivers online drop-in counselling, face-to-face group therapy, and peer support spaces. While these services are valued, they are not systematically funded and remain geographically uneven. Local councils operate mental health schemes, but access varies significantly by area. Volunteer organisations such as Samaritans and Barnardo’s offer volunteer support, but provision is case based rather than coordinated within a structured, culturally sensitive pathway.
We recommend enabling local councils to commission Ukrainian-led organisations such as OPORA under existing mental health funding streams to provide counselling, group therapy, and peer support in Ukrainian. GPs should be able to refer Ukrainian refugees with physical disabilities directly to these services, and to Ukrainian-speaking mental health professionals where available.
The Rapid Damage and Needs Assessments 4 and 5 (RDNA4 (2022-2024), RDNA5 (2022-2025)), produced by the World Bank, the Government of Ukraine, the European Commission, and the United Nations, assess damage and needs resulting from the war in Ukraine over the period from February 2022 to December 2025. They show that infrastructure damage remains severe after nearly four years of war. As of December 2025, total direct damage was estimated at US$ 195.1 billion, with housing, energy, and transport among the most heavily affected sectors. For disabled people, this damage is not only a matter of general reconstruction but radically effects their daily life. Safe return depends not only on security, but also on the availability of accessible housing, reliable electricity and heating, functioning transport, safe water and sanitation, healthcare, rehabilitation, and local support in the places to which people may return. RDNA5 identifies disabled people as one of the groups most affected by the war and notes that both the prevalence and severity of disability are increasing.
Disability certification systems differ between Ukraine and the UK. Most of our participants were required to re-confirm or re-prove their disability in the UK. For individuals from occupied territories, returning to obtain documentation is either impossible, unsafe, or extremely slow. Delays in confirming disability status can interrupt access to treatment, rehabilitation, and benefits, which negatively affect health outcomes. Legal specialist immigration advisers at Settled report that barriers also arise within the Ukraine Permission Extension process, including rigid biometric requirements, digital-only immigration status systems, strict documentation rules, and limited communication routes in complex cases. In practice, these problems have contributed to delays, benefit disruption, and additional risks for medically vulnerable applicants. The UK should accept existing medical evidence where possible, speed up disability-related decisions, and prevent visa changes from cutting off healthcare, rehabilitation, or disability benefits.
Ukrainian refugees with physical disabilities in the UK represent a clearly defined group (around 3-4% of the Ukrainian refugee population in the UK (DWP 2025, personal communication; ONS, 2023 personal communication)). Over three-quarters (76%) of our study participants originated from Ukrainian cities experiencing active hostilities, occupation, destruction, or regular air strikes (Appendix). Medical infrastructure in these regions has been destroyed or is unsafe. Access to rehabilitation, specialist care, assistive devices, and medication is severely limited or unavailable. Many of our participants had physical or mobility-related disabilities, meaning that inaccessible housing, transport, and healthcare infrastructure in Ukraine would significantly limit their ability to return safely or access essential service (MinRegion 2025, personal communication). Most of our participants rely on UK-based rehabilitation services, ongoing specialist consultations, regular medication, mobility aids and adapted housing. Under the current temporary visa arrangements, uncertainty about future status creates instability in employment, healthcare, and housing. Refugees with physical disabilities are also likely to face particular challenges in meeting any skilled employment criteria required under the new proposed settlement regulations.
For those with permanent physical disabilities who depend on UK-based treatment, rehabilitation, and adapted housing there should be a clear recognition of this when considering the rights of refugees from Ukraine to remain in the UK. Long-term right to remain in the UK needs to consider the specific circumstances of physically disabled Ukrainian refugees.
We are currently collecting data, with new documents and analyses to be uploaded here.